Ky. study shows syringe exchange programs decrease infections associated with IV drug use, could result in ‘big money saved’
By Melissa Patrick
Kentucky Health News
A new analysis of Medicaid claims data suggests that Kentucky counties with syringe-service programs have slightly lower rates of diseases associated with intravenous drug use, such as HIV and hepatitis C.
The analysis estimated a progressive reduction of 0.5 percent per month, adding up to a 6% increase over a year. That can add up to savings, not only in lives, but money. So said Dr. Connie White, deputy commissioner of clinical affairs for the Kentucky Department for Public Health, at the Kentucky Harm Reduction Summit Aug. 20.
White said, “As a public-health person, I think of all the emotional tragedy for the patient and for the family with one of these co-morbidities,” diseases and conditions that occur together. “But if you’re trying to sell this program to a bunch of politicians and legislators, you’re talking about money saved, we’re talking big money saved.”
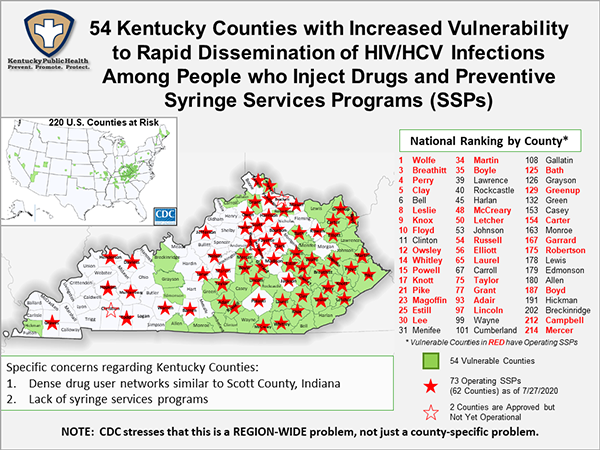
Kentucky has more syringe-service programs than any other state in the nation, but 56 of the state’s 120 counties still don’t have one — and 20 of those are considered highly vulnerable to an HIV or hepatitis C outbreak among IV drug users, according to the Centers for Disease Control and Prevention. Thirty-four of the state’s most vulnerable counties have operational syringe exchanges.
The vulnerable counties without an exchange include Bell and Clinton, which rank sixth and 11th on the national list of 220; Cumberland, Casey, Edmonson, Harlan, Johnson, Lawrence, Lewis, Menifee, Monroe, Rockcastle and Wayne, also in Appalachian Kentucky; and eight in the rest of the state: Carroll, Gallatin, Green, Breckinridge, Grayson, Green, Allen and Hickman.
Kentucky has 74 operational syringe-service programs in 63 counties, with one more in Christian County approved but not operational. Bracken County’s exchange is marked on the state’s map as not yet operational, but it started operating July 8.
Syringe-service programs are more broadly referred to as harm-reduction programs and are designed to prevent outbreaks of HIV and hepatitis C, which are commonly spread by needle sharing among IV drug users. They also provide health screenings and vaccines, and connect drug users to treatment.
They are allowed by a 2015 state law that requires approval by the county health board, the fiscal court and the city where the exchange is to be located.
Syringe exchanges reduce disease
The Kentucky Office of Health Data and Analytics did the analysis at the request of the Department for Public Health.
One reason the study is so important is that it helps to root the debate about such programs in empirical data, said Mathew Walton, a researcher with the office.
Walton pointed to a national study that shows a person’s political affiliation, income, and amount of stigma they feel about addiction and syringe-service programs are significant predictors of whether or not someone supports these programs — not the facts.
The study looked at Medicaid claims from January 2015 through June 2019 in any county that had implemented a syringe-service program during that time.
It looked for six infections largely connected to IV drug use and minimally associated with other activities: HIV, hepatitis C, endocarditis, osteomyelitis, and, in people diagnosed with opioid-use disorder, skin and soft-tissue infections. The researchers only included new infections in their analysis.
The study looked at infection rates before and after the syringe exchange was established in 42 counties. Recognizing that results might not be seen immediately, included lag times of one month, three months and six months. It also adjusted for a list of variables, many related to demographics.
Cameron Bushling, a statistician with the office, said each of the lag-time scenarios showed a decrease in infections after the syringe exchange was established.
“The infection rate in your county will go down by roughly half a percent each month after you implement a syringe service program,” he said. “So some, some may think this is a small number, but it’s important to keep in mind that our infection rates were very low. . . . So half a percent is still a pretty big find.”
In conclusion, Walton pointed out that most of the counties in the study were rural, outside metro areas.
“There’s an evidence of an association that they were successful in reducing infection, new infections,” Walton said. “These do seem to be an effective use of resources for preventing costly and harmful infectious disease.”
He said the savings would come with even small reductions in infections caused by IV drug use.
“While this analysis revealed that this set of infectious-disease diagnoses was rare, even preventing a small percentage of them can have a significant effect on the Medicaid program,” he said. “A single course of treatment for hepatitis C can be as much as $85,000 or more, so even a small outbreak prevention can be both a sort of economic benefit as well as a humanitarian and medical population health benefit.”
“Well, first, just don’t give up,” he said. “Second, do everything you can to get the public on your side, the voters on your side. . . . and continue to keep raising this issue.”